Millions of alarmed Americans, and people the world over, grabbed the nearest bludgeon to fend off the Trump presidency. They reached for anything handy: street marches, sympathetic pundits, counter-tweets, progressive infotainment, social media. Unfortunately, most of these reactions only fed a vicious cycle of attack and counter-attack.
For the relatively few psychiatrists and other mental health professionals who took up arms, the bludgeon readily at hand was psychiatric diagnosis and a self-proclaimed “duty to warn.” Hastily written petitions and books preached to the choir. If you already knew Trump was disturbed, here was confirmation by experts.
The converse was also true. If you believed the left played underhanded tricks to disempower a democratically elected President, these statements were your proof as well. Condemnation of Trump by woolly-headed liberal therapists was hardly news. It simply confirmed that educated elites are not above it all. We merely chant our political slogans in fancier language.
The warrior psychiatrist
A prominent voice in this chant was Bandy X. Lee MD, a psychiatrist affiliated with Yale University who helped organize a small conference to discuss Trump’s mental state — the “Duty to Warn” conference — and who later authored the bestseller, The Dangerous Case of Donald Trump: 27 Psychiatrists and Mental Health Experts Assess a President (Thomas Dunne Books, 2017). Dr. Lee published an expanded edition in 2019, and another book about Trump in 2020.
Positions like Dr. Lee’s led to wide debate over the “Goldwater Rule” of the American Psychiatric Association (APA). This ethical standard prohibits APA members from issuing a professional opinion about a public figure’s condition unless the psychiatrist has conducted an examination “and has been granted proper authorization for such a statement.” During the Trump administration the APA defended this standard, while others, including Dr. Lee, held that a duty to warn the public superseded it.
In reality, most of the debate over the Goldwater Rule was moot. The Rule only applies to members of the APA. Dr. Lee is not a member. Nor, of course, are the vast majority of mental health professionals who are not psychiatrists. The ethical standard of a voluntary membership organization is hardly the “gag rule” Dr. Lee and others claimed.
No constitutional right to teach at Yale
However, other “gag rules” hit closer to home. As reported this week in the New York Times, Yale canceled Dr. Lee’s volunteer faculty position last year after colleagues warned that her public statements called into question her “clinical judgment and professionalism.” Dr. Lee then sued Yale, alleging that her dismissal violated her First Amendment rights and impinged on her academic freedom.
The courts will decide the merits of her case. However, on the face of it, Yale has not prevented Dr. Lee from writing or speaking. The First Amendment protects speech from government restriction, not from deplatforming by a private university. Indeed, Yale has countervailing First Amendment rights of its own.
It is also worth emphasizing that Dr. Lee had a non-tenure, volunteer faculty teaching position. I have held such positions myself throughout my career. A psychiatry department’s decision to use or not use someone to teach trainees often boils down to subjective personality factors. If an instructor has an “agenda,” or brings unwanted controversy to the department, that alone may be enough to end the affiliation.
Do we help or hurt?
The bigger question, which goes well beyond Yale’s choice of teaching faculty or a rule for APA members, is whether academically-toned denunciations of political figures by mental health professionals add anything to political discourse.
The practical implications seem quite limited. Dr. Lee’s books didn’t move the needle. They merely fed the the cycle of attack and counter-attack. Trump’s critics and supporters alike found confirmation of their prejudices. Moreover, Americans were again reminded that our means of removing a sitting president — impeachment and invoking the 25th Amendment — are political acts, not governed by medical or psychiatric wisdom. Diagnosis is a sharp instrument for helping patients, but at best a blunt weapon in politics.
Psychiatric outcry can do very little, whether in the court of public opinion or the actual machinations of government. Ours is one small voice in a sea of voices, all clamoring to be heard.
Risk of self-harm
Meanwhile, there’s a real risk of self-harm to the mental health professions. When we make dubious claims to authority, we appear smaller not larger. When we trade professional integrity for momentary media coverage, the whole field suffers.
Worse, we may unwittingly invite a dystopia where all political factions deploy mental health experts to declare their opponents unfit. A cacophony of warnings to shun the allegedly unbalanced — the very thing misguided psychiatrists did to Senator Goldwater in 1964 — bodes poorly for a democratic process premised on voters making independent assessments of character. Such warnings are also the very definition of an ad hominem attack. Little surprise Yale drew the line.
Image courtesy of bplanet at FreeDigitalPhotos.net
In the months since the COVID-19 pandemic forced me to practice by video and phone, I’ve exchanged much more email with patients than I did before. Previously, I discouraged email from patients. For one thing, I knew it was an insecure channel, not “HIPAA-compliant.” It’s also somewhat less personal than a phone call. But starting last March I gave patients my work email, which they needed in order to connect to my video link (usually Doxy.me) for sessions. Most also use it to pay me online. Perhaps inevitably, email has become the most convenient way to send short messages back and forth, mostly medication refill requests and appointment confirmations or changes.
Due to the pandemic, I also linked an online version of my intake form to the front page of my website, so new patients could complete it remotely. The completed form was transmitted to me by non-secure email as well.
As the months dragged on, I realized I needed to treat all this electronic communication more carefully. I started researching secure email designed for medical practices. Below I’ll tell you what I found.
What is HIPAA-compliant email?
But first, a brief dive into terminology. HIPAA, short for the Health Insurance Portability and Accountability Act of 1996, is a federal statute that, among other things, regulates the secure sharing of medical information, especially electronically. Those of us who traffic in “protected health information” (PHI) — “covered entities” such as doctors, hospitals, clinical laboratories, insurance companies, and others — must store and transmit PHI in secure ways. We also sign “business associate agreements” (BAAs) with each other. A BAA is basically a contract that says covered entities will only share PHI with other covered entities.
While many people assume HIPAA exists to assure privacy, the law actually arose to facilitate electronic information exchange, often without the patient’s explicit consent. For example, HIPAA allows behind-the-scenes sharing of PHI to “coordinate care.” But for purposes of this review, I’ll focus on the privacy safeguards, not the many other parts of HIPAA.
To be HIPAA-compliant, email must be protected at both ends, e.g., with passwords, and engineered to prevent interception and reading en route. Technically, HIPAA does not demand that email be encrypted (translated into unreadable code), although that is typically the strategy used. The email provider and the covered entity using that provider should sign a BAA.
Regular email, in contrast, isn’t designed to be secure. Messages are copied in readable form from one internet node to the next. Bad actors can intercept them along the way.
What I found
So who offers HIPAA-compliant email? One option are companies that provide complete electronic practice management systems. These typically include secure messaging with patients as part of their larger range of services. I didn’t deeply research this, as I’m not in the market for such a system. Using one solely for secure messaging seemed too expensive, unwieldy, or both. But I did briefly look into ChARM EHR and Luminello, both of which include secure communication with patients, and offer a free version with limited features to try out. ChARM is designed for all types of small medical practices, not just mental health, while Luminello is for mental health only, including non-medical therapists and “wellness clinicians.” Perhaps thanks to its specificity, I found Luminello much more user-friendly; I’d seriously consider it if I were in the market.
But I’m not, so I turned to free-standing email services.
Best I can tell, all HIPAA-compliant email is actually webmail. That is, the recipient receives a regular email with a link to a secure website to pick up the message. Services differ with respect to email storage, often 1 to 5 gb; ways that non-subscribers, e.g., patients and potential patients, can reach you securely; whether you can use an existing email address versus having to get a new one; and whether you can choose an email address from a website domain you own (e.g., therapist@mycompany.com). All include a BAA.
Several companies provide secure email to larger clinics with multiple clinicians, administrative staff, and maybe a dedicated IT person. They usually charge monthly fees to match. That’s not my situation, and I do not review them here. Instead, here are a few sized for the solo practitioner:
Hushmail for Healthcare (www.hushmail.com) – $109/yr: Pros: Secure forms submission, with two nicely customizable forms at the above price. 10 gb storage. Can use your own domain for email. Cons: Can’t use an existing email address in a domain you don’t own (e.g., gmail, hotmail, yahoo, etc). The price doubles for more forms.
MailHippo (www.mailhippo.com) – $60/yr: Pros: Arguably slightly stronger encryption than Hushmail (AES 256 bit versus OpenPGP). Can recall an email message, for example if addressed incorrectly. Uses your existing email address. Includes a personal URL so anyone can send you a secure email; adding this URL to your website, or to your signature at the bottom of regular email, invites secure messages from others. Cons: No forms.
MD OfficeMail (www.mdofficemail.com) – $23/yr with their email address, $32/yr with your own Pros: Cheapest paid HIPAA-compliant email I could find. Includes a personal URL so anyone can send you a secure email. Cons: User interface is old and clunky. No forms.
The following offer encrypted email — and are based in Europe, not the US — but are not designed for HIPAA specifically, i.e., no BAA:
ProtonMail (www.protonmail.com) – Free, or $48/yr for more features and email storage Tutanota (www.tutanota.com) – 12 euro/yr for “business,” free for “private.” Includes a secure calendar and address book, which would make Tutanota my choice if I merely wanted these encrypted features for personal use.
There are also a number of free, ad-supported apps that will encrypt email on handheld devices. These aren’t HIPAA-compliant either.
And the winner is… my patients
In the end I decided to go with Hushmail, mainly because it offered the secure forms I needed: a general contact form and an intake form for my website. I also was able to use my own web domain (@stevenreidbordmd.com) for my new email address. If I hadn’t needed the forms, I would have chosen MailHippo instead, to keep my existing email address.
Once signed up, I converted the contact form and intake form on my website to Hushmail. Then, using my old, unsecured email, I sent a final message to my active patients asking them to stop using that address, and to expect secure email from me going forward. Since replying to a secure email also makes the reply secure, this is a good way to start a private, HIPAA-compliant email channel with each patient.
One of the best uses I’ve found so far for secure email is sending monthly billing statements electronically, as pdf attachments, instead of by mail. If patients or potential patients want to reach me securely before I send them anything, they use the contact form on my website to start the exchange. So far, my new system has been working well.
In the comments below, let me know how any of these solutions work for you, or if you have others to recommend.
Image courtesy of Stuart Miles at FreeDigitalPhotos.net
Back when traumatic experiments on animals weren’t ethically prohibited, human anxiety was modeled by subjecting lab animals to an irresolvable approach/avoidance dilemma. The oldest and bestknown example came from researchers in Ivan Pavlov’s laboratory. They classically conditioned dogs to associate food rewards with the sight of a circle, and also trained the same dogs to associate ovals with not getting food. Once trained, the dogs were shown ovals that looked more and more circular, until eventually they couldn’t tell them apart. At that point, the animals became acutely agitated.
This paradigm became known as experimental neurosis. It was offered as a behavioral account of neurosis at about the same time Freud was developing a psychoanalytic account. Experimental neurosis could be induced in many different species, and via both classical and operant conditioning. As an example of the latter, thirsty lab rats were given access to a metal water spout with an electric charge. The rats wanted the water, but didn’t want the shock. As a result, the rats had physiologic and behavioral reactions that looked a lot like human anxiety.
Many of us wince even at the description of these experiments. We empathize with the poor creatures confronted with an irresolvable problem. Nowadays, the experiments seem cruel, even though the goal was to relieve human suffering (e.g., the rat studies were done to test anti-anxiety medications before trying them on people).
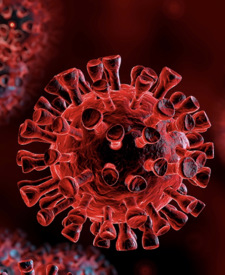
The coronavirus pandemic challenges us with similar approach/avoidance dilemmas, leading to what we might call “COVID-19 neurosis.” Nearly all of us are strongly inclined to interact physically with others. We have lifelong associations of human touch and closeness with comfort and safety. Parents hugging children, lovers kissing, friends whispering comments from mouth to ear; hands on shoulders, playful roughhousing, gentle caressing: these and countless other acts of intimacy are high points in our emotional lives. They are undeniably rewarding — like meat to the dogs and water to the rats.
COVID-19 has made each of these aversive: it electrifies the water spout. Every physical encounter risks a potentially fatal disease. The threat looms even when the statistical likelihood is small; public warnings blare to shake us from our usual habits. Acts that used to be caring, comforting, or simply friendly are now threatening. We refrain from touching our grandparents. We steer clear of others on the sidewalk. In-person medical care may leave us sicker than when we arrived.
Coupling reward and punishment to the exact same behavior is crazy-making. No wonder so many of us have gone from anxious to depressed as the pandemic wears on. Indeed, that’s exactly what Pavlov described in many of his dogs: eventually the agitation died down and they gave up.
In this case, though, giving up leads to more sickness and death. The sad truth is that all infectious diseases, not just COVID-19, specifically exploit our social nature. There would be no contagion if we each lived in our own bubble. Pathogens unthinkingly, mechanically capitalize on the very traits that most make us human. That’s literally how they work.
It’s tempting to call this cruel, as though we suffer at the hands of an evil scientist torturing dogs or lab rats. Victimization leads many of us to point fingers at villains — rule mongers, rule breakers, the privileged, the needy — who represent this cruelty in our minds. But we’re not being punished, not really; no more than earthquakes or tornados punish us. The natural world has consequences. The virus doesn’t care about our political philosophy regarding masks, or whether we’re usually kind to strangers. It only cares about infectivity, immunity, and the now famous R0.
One thing Freud had over Pavlov was a cure for neurosis. But we don’t need psychoanalysis for the experimental neurosis caused by COVID-19. Unlike dogs and rats, we can understand the problem, imagine a future after the pandemic, and delay now-risky gratifications until then. It’s not easy or fun, but a number of countries have shown it’s possible. It demands imagination and will, accepting reality, and not taking the affront personally.
I’m increasingly asked by patients and potential patients when I plan to see people in the office again. I had been an exclusively “in person” psychiatrist and psychotherapist until mid-March of this year, when the pandemic forced even skeptics like me to convert completely to remote (“virtual”) treatment. Like many of my colleagues, over the past three months I’ve made an uneasy peace with phone and video sessions, and all the accompanying rigmarole. Although I can work with it, it’s far from ideal. I look forward to dispensing with the earbuds and glitchy bandwidth and resuming my prior practice.
While some folks hope I’ll see them in the office right now, others fear I’ll “force” them back before it feels safe. I assure them I won’t. Even when the office reopens, I anticipate a hybrid situation for months to come, a combination of office and online appointments. Normality is a long way off.
After all, risk tolerance varies. Some of my fellow San Franciscans now share walks outside without masks — nominally six feet apart, but not always — and some are again dining in outdoor cafes. Others are not. Even leaving aside political theater and virtue signaling, reasonable people can disagree about what feels safe.
While it would be comforting to ascribe differing risk tolerance solely to logic and the biologic, e.g. older people are at higher risk, it is far more subjective than that. Partly it’s self-image: are we proud of being sensible and prudent, or fearless and no-nonsense? Are we the type to cite scientific studies, or our gut? Do we sacrifice on behalf of others, or believe only bleeding-hearts do that? Partly it’s modeling by others, variously called peer pressure or social learning theory. If everyone nearby wears a mask, we’re more comfortable wearing one; if others reopen their therapy offices, we’re more apt to reopen ours.
The arbitrary way most of us make these safe/unsafe determinations also reflects wishful thinking and confirmation bias, cognitive tricks we play on ourselves to rationalize unsafe behavior — or conversely to scare ourselves when the situation isn’t that bad. “COVID-sorting” is essentially the use of prejudice and stereotypes to make safety assessments. We’re loath to see our own decision-making in such unflattering light, but of course we readily see irrationality in the fools who decide otherwise.
I’ve been in online discussions with mental health professionals across the country. Some are actively strategizing how to medically screen patients at office entrances, how to disinfect surfaces between patient appointments, how to conduct sessions while masked. Others sound pessimistic about ever going back to the office. I imagine this variation isn’t unique to my field. It was far easier to hunker down uniformly a couple months ago than to customize a re-emergence now.
Adding to the challenges faced by many businesses are special considerations for therapy practices, where feeling safe is crucial. Psychotherapy can only happen when words can be said and reflected upon without harmful real-life consequences. It exists in name only if either party fears a potentially fatal illness in the encounter. Indeed, it’s the therapist’s duty to assure safety in treatment, which is why our ethics forbids sexual and other forms of exploitation. The same rationale obliges therapists to take reasonable steps to assure the safety of both parties from viral and other medical threats.
And if that weren’t enough, these practical matters pale in comparison to the realm of fantasy, where under normal conditions patients may imagine the therapist to be benevolent or evil, soothing or toxic, and themselves impervious or vulnerable, lovable or repulsive. When explored as transference fantasy, these reactions can lead to insight and change. However, when toxicity and vulnerability stem from actual health risks, their value as guideposts to the unconscious is lost.
Ultimately, my answer regarding reopening the office hinges on inertia — my willingness to take the necessary steps — and practicalities, not unconscious fantasies. Will doing so necessitate calling patients the night before to screen for illness? Checking their temperature at the sidewalk entrance, one floor down? Supplying hand sanitizer and spare masks, posting signs, cleaning chairs and other surfaces between appointments, keeping office air flowing with fans and open windows?
Is this rigmarole preferable to the rigmarole of online intake forms, frozen video feeds, garbled audio, and occasionally needing to switch to the phone halfway through a session? It’s hard to choose between two bad options. And even if I decide “in-person” is preferable, will many of my patients concur? While it was my decision to exclude them from my office in March, it will not be my decision alone to readmit them.
Deciding when to reopen a therapy office isn’t only a question of risk tolerance. It’s balancing risk against expected benefit — two subjective estimates — and weighing competing rigmaroles. Even as a fairly risk-tolerant person, I am not ready to reopen my office just yet. By my estimate, the calculus still favors waiting to reopen another day. I only hope that, somehow, that day comes soon.
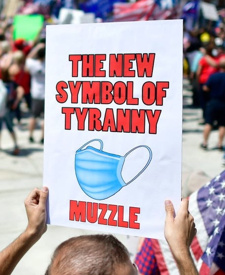
But let’s be fair and make some distinctions. At one extreme are those who deny reality. A few conspiracy theorists hold that COVID-19 is a hoax, or more narrowly that it is real but overstated by political opponents, in order to hurt Trump’s presidency and re-election bid. It’s a psychological curiosity to maintain such claims in the face of photographic evidence, first-person accounts, a large number of certifiably dead people of all political persuasions, and so on.
Lately the objections have shifted somewhat. Many protesters now argue that masks don’t help: that they don’t stop the virus, or that they even increase risk by leading wearers to touch their faces more often. These claims, too, fail in the face of science as well as common sense. No one normally objects to covering a sneeze or cough.
Then there are subtler objections. It’s true, for example, that Americans valorize risking one’s life in defense of freedom. Shouldn’t we similarly honor those who make the individual decision to be free, of masks and social distancing in this case, at the cost of increased infection risk? Isn’t this akin to taking up a risky sport, or volunteering for hazardous duty?
The difference, of course, is that masking and social distancing aren’t for the individual alone. These acts protect others. Like obeying speed limits and fire codes, the life you save may not be your own. For most of us who wear masks to fight the pandemic, not doing so seems selfish: a conscious choice to maximize one’s own freedom by imperiling others. We’re all in this together, we plead; do it for your neighbors and elderly relatives. New York governor Andrew Cuomo recently argued that wearing a mask shows respect for health care workers risking their lives, and for one’s fellow citizens. Unfortunately, in an age of tribalism, this sort of collectivist argument rubs some the wrong way.
There’s another dynamic at play here too. It may seem minor, but for the protesters it surely isn’t. Cuomo didn’t dwell on the concrete benefits of mask-wearing; he stressed what it symbolizes. A mask shows the wearer is respectful, virtuous. This argument sounds a lot like virtue signaling: a gesture to convey virtuous values without necessarily accomplishing anything.
Here’s another example. I’ve been wearing a cloth mask whenever I walk outside. Yesterday I was strolling several blocks to an outdoor market, where due to the lines and crowd I’d definitely need and want to be masked. But the sidewalks on the way were nearly deserted. I’d face no increased risk by breathing freely, nor would I risk anyone else. I wore the mask partly out of habit, and partly, I realized, to convey my righteous pro-mask stance. The latter is virtue signaling, as wearing a mask outside on a deserted city block offers no practical advantage. It inconvenienced me, and made it a bit harder to breathe, for no reason but symbolism and self-image. I took it off until I neared the market.
My sense is that many mask refusers are enraged by virtue-signaling. The populism that brought Trump to power actively rejects “I know better than you” statements and gestures, especially those laden with moral overtones and real-life costs. Yes, it’s childish in a “cut off your nose to spite your face” way. After all, wearing a mask in markets or stores really matters. One might say that self-defeating behavior is true of Trumpism in general — more about expressing visceral opposition than a considered alternative.
This didn’t arise out of nowhere. For years, the left has taken moral stands that strike the right as precious: saving whales, using the right pronoun, denigrating meat-eating and gasoline use, and so on. Let’s grant that each of these causes would make the world a better place in the long run. However, in the short run these admonitions can come across as scolding, elitist, and out of touch with everyday concerns. People react badly to that. The chiding sounds parental. Emotionally, it invites angry adolescent rebellion. To make matters worse, dismissing such reactions as hopeless or deplorable merely adds dead-dinosaur gasoline to the fire. It’s a bit like a parent telling a teen he’s a loser and won’t amount to anything.
In family therapy, there’s often an “identified patient”: usually a child or teen with overtly pathological behavior who expresses the whole family’s otherwise hidden dysfunction. In larger society, too, playing one type of “sensible” role may invite others to play a complementary role that looks more overtly pathological. Authoritarians breed rebels, codependents invite manipulators, and so forth. If an angry minority fights sensible public health measures using immature, self-defeating behavior, it’s wise to consider what’s provoking them. And to recognize that everyone, not just our political opponents, is influenced by emotional irrationality.
The answers to our sincere questions may be uncomfortable ones that implicate ourselves.
To be clear, no one should use psychiatric diagnosis to critique a political position. It’s a feel-good tactic that inevitably backfires. Some mental health professionals tried with Donald Trump, and only encouraged his defenders to lodge counter-charges of mental illness in more liberal politicians. When it comes to masks, it might be argued that the pro-mask majority are “anti-social” in a colloquial sense: we privilege scientific/medical theory over immediate human connection.
Pandemics have been with us through history. Likewise, resistance to pandemic masks isn’t new. Many arguments used today against masks were used a century ago in the 1918 flu pandemic. We know a lot more about viruses and epidemiology now than we did then, and the scientific rationale for masks and social distancing is stronger than ever. But social dynamics haven’t changed much. People still don’t like being told what to do, especially if there’s a suggestion they are willfully ignorant or morally deficient. It’s incumbent on those advocating pro-social behavior to make it a win-win proposition, and not a moral failing — or a psychiatric disorder — for resisting.
It was 2013. Hi-tech entrepreneurs were excitedly “disrupting” industries, bringing goods and services closer to users. Uber replaced cabs, Kickstarter replaced investors, and telehealth companies offered convenient, at-home medical care over smartphone video. Why waste time going to an office or clinic, especially if you’re not feeling well? Why spend so much money? The physician’s physical examination had been oversold. It wasn’t really needed.
Psychotherapy never required a physical exam in the first place, and so was even more ripe for disruption. Therapy, after all, is just talk. A phone call will do, although that lacks cutting-edge tech and huge potential profitability. Proprietary video channels solve those drawbacks. Therapy could be mass-marketed as a commodity more than a professional relationship, always available and as close as your phone. It was sold to the public with a fresh, slightly subversive undertone: fire your shrink and use our app. Have therapy at home, in your pajamas if you like. It’s even “evidence-based,” a sleight-of-hand that substitutes symptomatic improvement for truly feeling well.
In 2013 I was skeptical of the burgeoning popularity of online therapy:
When the alternative is no psychotherapy at all, the utility of conducting it online seems obvious. Example scenarios include patients who are bedridden or otherwise immobile, those in inaccessible locations such as Antarctic explorers, and those who are immunocompromised or highly contagious with an infectious disease…. It is more potentially problematic to choose online therapy over in-person treatment when both are practical options.
Back then, choosing online therapy over face-to-face struck me as corner-cutting: opting for fast food over fine dining. Yes, it was easy to imagine implausible conditions where the former was the best available or the only practical option. But that wasn’t the reality. Instead, online therapists and their patients chose convenience, the innate attractions of tech, and sometimes a lower fee, while settling for a substandard experience.
It’s 2020 now, and times have certainly changed. In the midst of the COVID-19 pandemic, it hardly ever makes sense to risk infection in the psychotherapy office. Conducting sessions by video, or simply over the phone, is much closer to standard therapy than it is to nothing — close enough that holding out for the real thing is recklessly rigid. Other things being equal, in-person therapy is still superior to the online variety. However, it isn’t so much better that it’s worth the risk of a potentially fatal disease.
This March, I offered all patients the option of telephone or video sessions instead of meeting in person. Most readily accepted. One or two had no private place to speak with me other than my office, so I continued to see them in person. Even our strict Shelter in Place order in San Francisco allows supermarket shopping, picking up take-out food, and visiting the dry cleaner or hardware store. Sharing my office for 50 minutes with one person quietly sitting eight feet away, when both of us are asymptomatic and I handle the doorknobs, didn’t seem out of line with these other common exposures; it was also permitted under the law. This week I decided to wear a cloth mask when seeing the rare such patient in the office.
Most patients opted for video. I tried FaceTime and Zoom before settling on Doxy.me. I found the three services essentially interchangeable, despite raging debates about HIPAA compliance and privacy. Audio and video quality varied a lot, though, depending on internet bandwidth. The calls improved substantially when I replaced wifi with wired ethernet at my end. But there were still occasional frozen video feeds and garbled audio. Once or twice it was so bad we switched to telephones mid-session. Conversely, when everything was going well, which was usually, the technology receded into the background.
Well, except that I was, and am, still conscious of positioning myself correctly in the camera frame, modulating my voice, attending to my facial feedback, confirming the novel payment arrangements, and asking about the transmission quality at the other end. I imagine all that improves with practice.
I considered charging less for phone and video sessions, maybe even less for phone than video. To my mind, I wasn’t offering as much virtually as I do in a “real” session. But I ended up keeping my usual fee, on the theory that my time and expertise are equally valuable no matter how it’s delivered. Of note, many insurers don’t see it that way. As of this writing, Medicare just started covering video therapy, but not telephone therapy (yet).
When the crisis is over, I plan to resume in-person services and retire the remote options. I fear others will not — that therapists and patients will have learned to accept glitchy transmissions and the other distractions of tech as normal. I worry, too, that therapists will no longer value the subtleties lost online: the quiet sighs, sly glances, and fleeting hesitations that add music and meaning to the words.
To my surprise, even the American Psychoanalytic Association blog argues that “online therapy can be just as effective as being in the same room with your therapist.” (This is not APsaA’s official position.) I wonder if this is a counterphobic reaction to psychoanalysis suffering a behind-the-times reputation for generations. Curiously, their argument is based on online music being emotionally moving. However, as noted by the general manager of New York’s Metropolitan Opera, the fact that online music is moving doesn’t mean it equals a live performance. The interaction between artist and audience animates the latter.
So it is with psychotherapy. If we reduce therapy to mere information transfer — complaints, feelings, and recollections in one direction, reframing, support, and/or interpretation in the other — then virtual therapy does a pretty good job. But if we see therapy as co-constructed, it’s more than information transfer. It’s “being with” each other in relationship. It’s intimacy. It’s closeness and trust.
Can this be approximated online? Sure. At a time when the viral risks of in-person treatment almost always outweigh its benefits, we should use the technology available to us. And third party payers should cover such sessions, which currently many don’t.
But when the dust settles, we’d be shortchanging our patients and ourselves if we settled for what we’re forced to champion now. The inconvenient truth is that physical exams are often important in medical diagnosis, and can’t be replicated online. Likewise, in-person psychotherapy enjoys advantages that distance therapies can’t touch. There’s no shame in admitting that, while advocating for a little less right now.
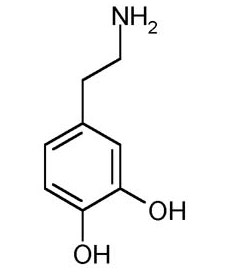
Taking a break from technology is a fine idea, but we don’t need a pseudoscientific new name for it: dopamine fasting. Launched with viral Silicon Valley memes, onlinereports, and articles in the New York Times and elsewhere, dopamine fasting is now a thing. Basically, the idea is to temporarily deprive oneself of the usual stimulations of life — largely electronic these days — in order to re-sensitize one’s brain.
Since several parties popularized the term, they wrestle over its definition. Some take an ascetic, globalview of stimulation-avoidance, while others limit the fast to electronic media. Getting too excited over these battles stimulates dopamine, of course. Perhaps it’s best not to worry about it.
Neuroscientists point out that the name is misleading. Dopamine isn’t uniquely implicated in habituation to stimuli or behavioral addictions (although it is certainly involved), and naming the neurotransmitter doesn’t advance our understanding of the process.
Consequently, it’s no surprise pundits debunk the idea as repackaged common sense. Sure, it’s refreshing to step away from the rat race and attention-grabbing tech. But we already have names for that: relaxing vacations, a “mental health day”, picturing your happy place, meditating, taking a walk to clear your head, the sabbath, sabbaticals, retreat weekends, and so on. The concept is as old as humanity. This, in turn, leads proponents to defend their baby with heartfelt but not entirely rational distinctions between dopamine fasting and these other activities.
I’m in the debunking camp. I agree with one of the vocal proponents of dopamine fasting, Cameron Sepah, who concedes: “The term is technically incorrect, but ‘stimulus control 101 for dealing with addictive behavior’ just doesn’t have the same ring to it.” In other words, the term “dopamine fasting” is hype, referring (with false, dopamine-inducing excitement) to an old, well-understood behavioral practice.
It’s also the latest example of misleading the public with whiz-bang neurobiological language. This is rampant in modern psychiatry, where the mere existence of functional brain imaging (allowing us to visualize metabolic activity in the brain) makes the field “biological” — even though our biological treatments haven’t improved as a result, and remain wholly symptomatic and empirical.
Attach a “neuro-” prefix or a brain chemical to your field of interest, and the world beats a path to your door. I recently joked that if we re-cast psychotherapy as “verbal neuromodulation” the field would enjoy newfound popularity and research funding. This is essentially what the advocates of dopamine fasting did.
Selling products with pseudoscience isn’t new. Old-time cigarette ads, believe it or not, touted their health benefits. Athletic clothing has been over-hyped to the tune of multimillion-dollar false-advertising settlements. Cosmetic ads frequently invoke essentially meaningless scientific terms.
The difference now is that social media has made the “marketplace of ideas” a real marketplace. Popularizing ideas, and by extension oneself, now demands the same promotional tactics previously used to sell cigarettes and soap. Can you, in some convoluted way, tie your idea to neuroplasticity? dopamine? cellular regeneration? If so, you’re well on your way to becoming an influencer. Yes, you’ll be pandering to the attention economy, and presumably stimulating and thus depleting everyone’s dopamine in the bargain. But don’t let that stop you.